

Introduction
The introduction of novel therapies has significantly improved outcomes in myeloma. However, the economic burden of enhanced healthcare utilization is significant and cannot be discounted. This study sought to identify baseline characteristics that may influence outcomes and subsequent healthcare utilization. Patients were also stratified by induction therapy to determine the impact newer combinations have on healthcare utilization.
Methods
This retrospective single-center study enrolled all newly diagnosed patients with myeloma between 2005 and 2020. Three outcome measures were used to determine healthcare utilization - total inpatient length of stay (LOS), number of admissions, and day ward attendances. Univariate and multivariable analyses were performed to identify significant covariates related to overall survival (OS) and healthcare utilization. Outcomes were subsequently adjusted for duration of follow-up and per patient year.
Results
There were 113 patients included; 60 (53.1%) female; median age at diagnosis was 67 years (IQR 62, 73 years) and 22.1% were high risk International Staging System (ISS). Further baseline demographics are presented in Table 1. Median duration of follow up was 3.2 years (IQR 1.50, 6.55). Sixty patients (53.1%) died, 91.7% attributable to myeloma or its treatment. Predictors of OS by multivariable analysis were advanced stage [ISS III (p<0.001)] and IgA idiotype [(IgA vs IgG) (p=0.0002)]. Stem cell transplant eligibility was associated with improved OS (p=0.003).
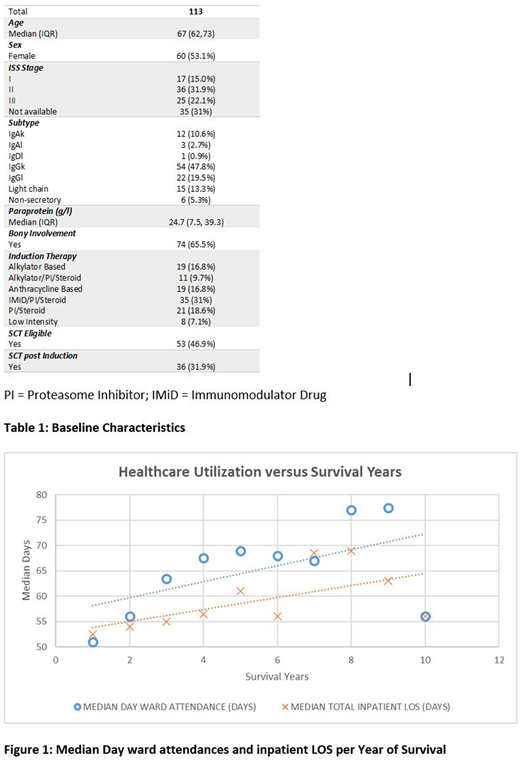
The total number of admissions to hospital was 547 (median 4; IQR 2, 7), with 55.4% unplanned. In the multivariable analysis, younger age (p=0.020), higher paraprotein levels (p=0.045), dialysis (p=0.037), and SCT eligibility (p=0.0012) were predictive of greater number of admissions. During the study period, there were 7000 inpatient bed occupancy days (median 46; IQR 26, 80). Only younger age remained significant (p=0.0028) in the multivariable analysis. There were a total of 5987 day care attendances during the study period. Multivariable analysis identified younger age at diagnosis (p<0.0001), WBC (p=0.0072), and light chain (kLC vs lLC) (p=0.0027) as predictive of increased day ward attendance. Healthcare utilization correlated with increased survival, as depicted in figure 1.
There was no significant relationship between treatment type and LOS (p=0.055); this remained unchanged when adjusted per patient year (p=0.24). There was significant relationship between treatment type and total number of admissions (p=0.015). Patients receiving anthracycline based therapy (p=0.003), Immunomodulatory (IMiD)/Proteasomal Inhibition (PI)/Steroid (p=0.020), or PI/Steroid (p=0.021) were more likely to have a greater number of admissions. However, when adjusted per patient year, this association was no longer evident (p=0.19). A highly significant relationship between treatment type and day ward attendances was identified (p<0.0001). Alkylator based (pp=0.005), alkylator/PI/Steroid (p=0.006), anthracycline based (p=0.0002), IMiD/PI/Steroid (p=0.0007), or PI/Steroid (0.0002) were more likely to have greater day ward attendance. When adjusted per patient year, this significant association between treatment type and day ward attendance remained (p=0.0002).
Conclusion
Studies assessing healthcare utilization in patients with myeloma are mostly limited to relapsed refractory setting. In this population, younger age at presentation was a significant predictor for all three measures of healthcare utility. Whilst treatment type did not demonstrate a significant impact of LOS, we did determine that novel triplet therapy combinations were associated with increased number of admissions and day care attendances. We also showed that healthcare utilization increased with survival time.
While survival outcomes with novel agents have improved, given current financial and capacity limitations within which the majority of health systems function, resource demand implications must be considered when planning future service provision and novel treatment strategies.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal